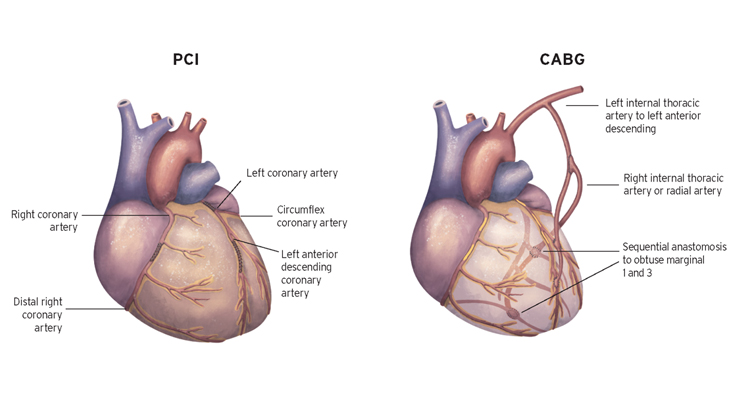
The most important trial of CABG versus PCI is the SYNTAX Trial.
SYNTAX was a trial in patients with multi-vessel and/or left main stem disease.
SYNTAX also had a database called a nested parallel registry that looked at outcomes in 1,078 patients who were deemed ineligible for randomisation for the SYNTAX study. Over 80% of the patients in this registry had coronary artery disease of such severity that it was considered they would not be appropriate candidates for stenting and were therefore referred directly for CABG. Only 16% of the registry patients actually underwent PCI having been deemed prohibitively high risk for surgery.
Overall, at one-year, the main result of SYNTAX was that repeat revascularization was much higher for those patients undergoing stent implantation compared to surgery(5.9% vs. 13.5%; P<0.001).
Overall, at five-years, stent implantation/ PCI failed to reach the pre-specified criteria for non-inferiority. In 1095 patients with three-vessel CAD, CABG reduced the risk of death (9.2% vs. 14.6%; P=0.006), MI (3.3% vs. 10.6%; P<0.001) and need for repeat revascularization (12.6% vs. 25.4%; P<0.001) without an increase in the risk of stroke (3.4% vs. 3%; P=0.66).
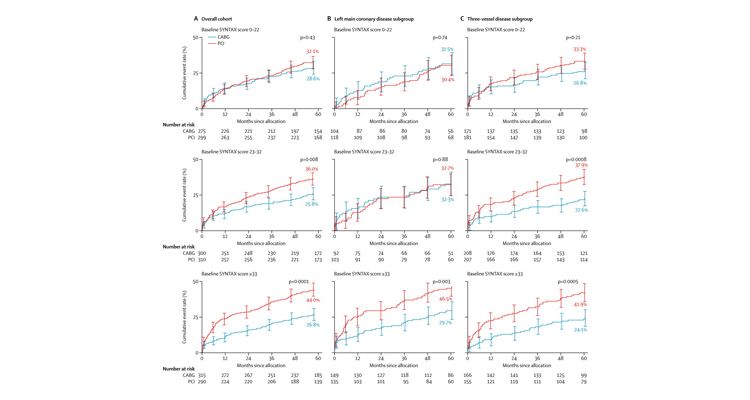
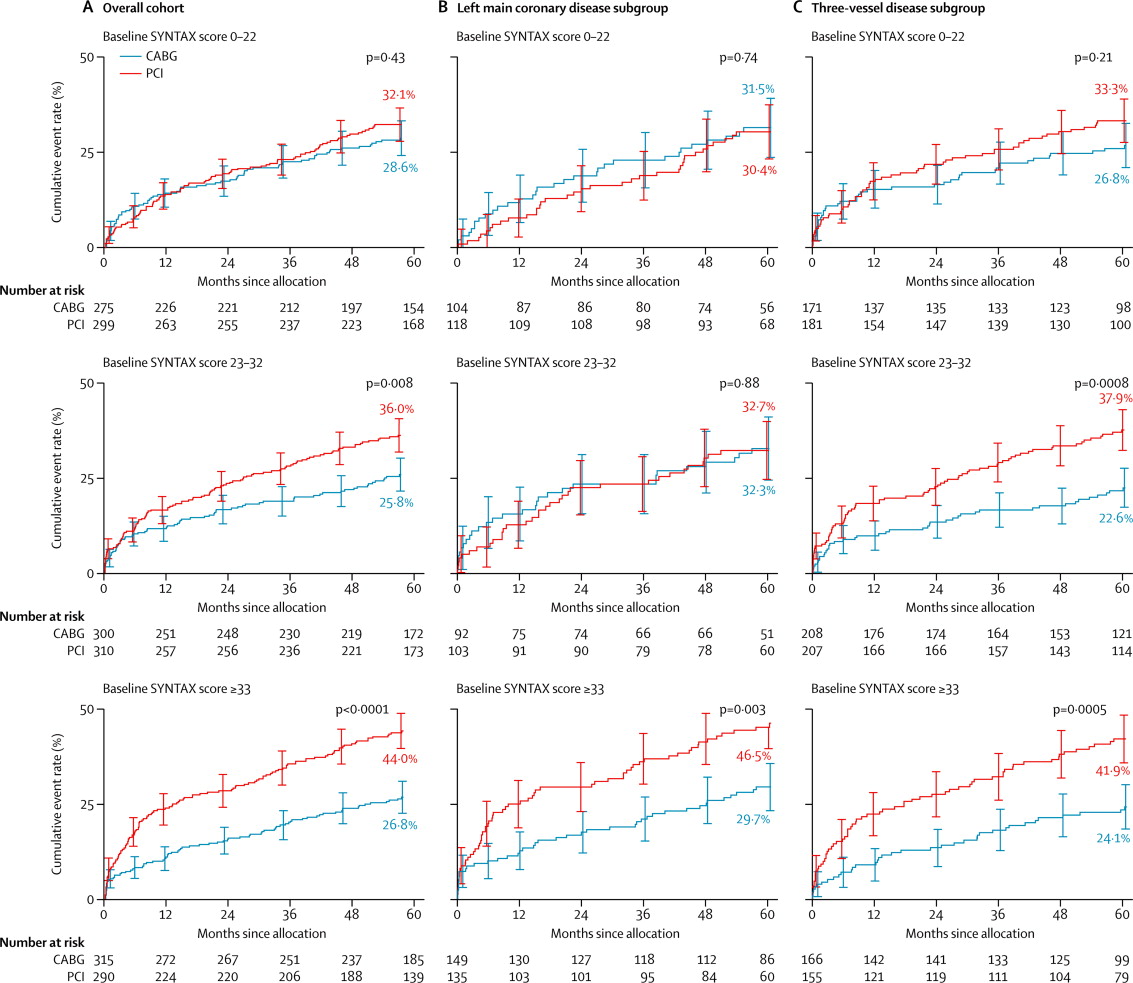
When analyzed by severity of CAD, as judged by SYNTAX scores, patients with intermediate (between 23-32) and higher (>32) scores had an absolute survival advantage with CABG as well as highly significant reductions in the incidence of MI and need for repeat revascularization.
Only in those with scores <22 was there a similar mortality between CABG and PCI, although CABG still resulted in significantly fewer MI and repeat revascularization.
This is an important distinction as 79% of all patients with three-vessel CAD in SYNTAX (1,095 in the RCT and 570 in the registry) had SYNTAX scores >22.
However, when the SYNTAX results are analyzed according to patients with left main disease a different pattern of emerges. In contrast to the situation for three-vessel CAD the respective 5-year rates of death (14.6% vs. 12.8%; P=0.53) and MI (4.8% vs. 8.2%; P=0.10) were similar whereas CABG had a lower risk of repeat revascularization in patients with SYNTAX scores less than 32.
In patients with SYNTAX scores >32 CABG resulted in lower mortality (14.1% vs. 20.9%; P=0.11) and the need for repeat revascularization (11.6% vs. 34.1%; P<0.001).