The natural history of chronic aortic regurgitation is well recognized. The asymptomatic patient who has moderate to severe aortic regurgitation may not have symptoms for many years. In seven studies,1–7 490 asymptomatic patients with moderate to severe aortic regurgitation were followed for a mean of 6.4 years. Based on these studies, the following can be concluded about asymptomatic chronic aortic regurgitation with normal left ventricular systolic function (i.e., an ejection fraction of 50 percent or greater)8:
In patients with asymptomatic chronic aortic regurgitation and left ventricular dysfunction, the rate of progression to symptoms is higher than 25 percent per year. In symptomatic patients, the mortality rate is greater than 10 percent per year.8
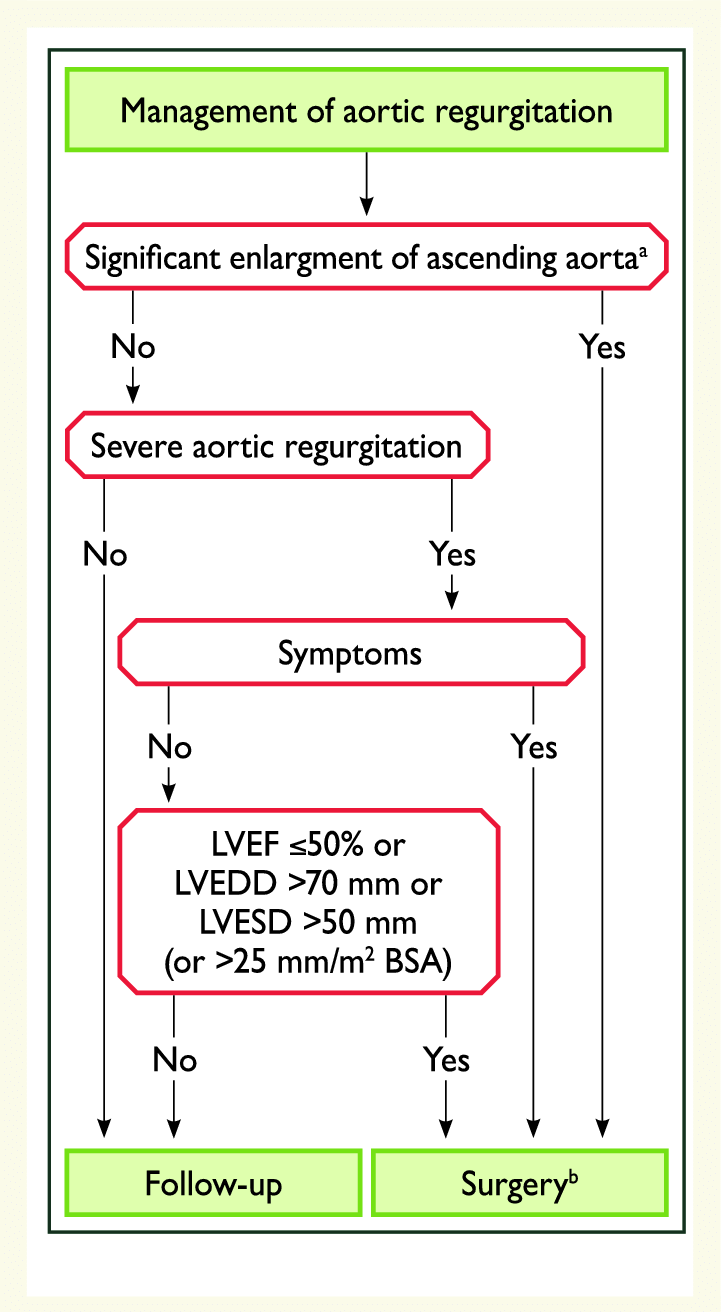
Although there is only a small chance of sudden death or left ventricular dysfunction in patients with asymptomatic chronic aortic regurgitation, these adverse events are possible. Therefore, it is important to follow asymptomatic patients for the development of symptoms and to examine them regularly to detect progression of severity. In addition, periodic quantitative evaluation of left ventricular function is necessary in patients with moderate to severe aortic regurgitation. When the history of exercise tolerance or symptoms is equivocal, exercise stress testing can be helpful.
The presence of aortic regurgitation, even when it is moderately severe, is not necessarily an indication for surgery. When surgery is needed, aortic valve replacement or repair, is usually required. Prosthetic valves, whether mechanical or biologic, have problems with durability, paraprosthetic leaks, thromboembolism and increased susceptibility to infective endocarditis. The decision to replace the valve requires that these potential problems be considered to represent less danger to the patient’s well-being than continuing medical management.
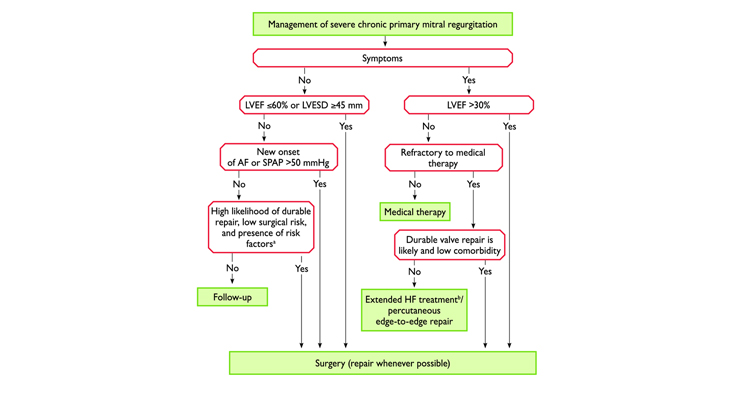
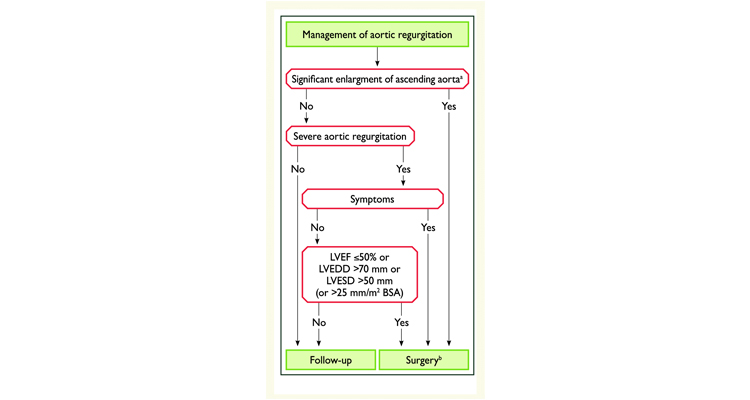
When should surgery be done for Aortic Regurgitation?