The best option is to try and preserve the existing valve. Doing this means that you won’t have to take anticoagulation drugs like warfarin for the rest of your life, and evidence shows that it reduces the risk of valve-related complications in the future.
Aortic root reconstruction without valve replacement is done because not all aortic root disease is accompanied with aortic valve dysfunction. Yacoub, in 1983, and David, in 1991, separately devised procedures that spare the native aortic valve, called, valve-sparing aortic root replacement. During the reimplantation procedure, a surgical tube graft is fixed at a level proximal to the annulus, to the tissue of the left ventricular outflow tract. Since the origin of the David procedure, there have been multiple modifications to the technique with the latest emphasizing restoration of the sinuses of Valsalva by the creation of neosinuses. Special grafts with sinuses (Gelweave) are also available. Dr Babar Bashir CHAUDHRI is an expert in these techniques, having trained in MHH, Hanover, Germany.
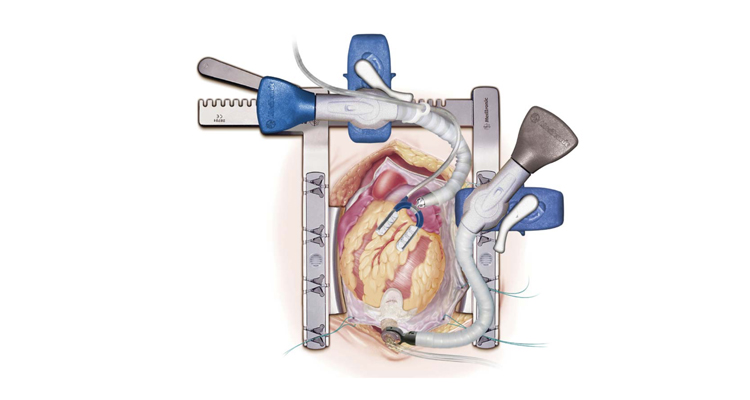
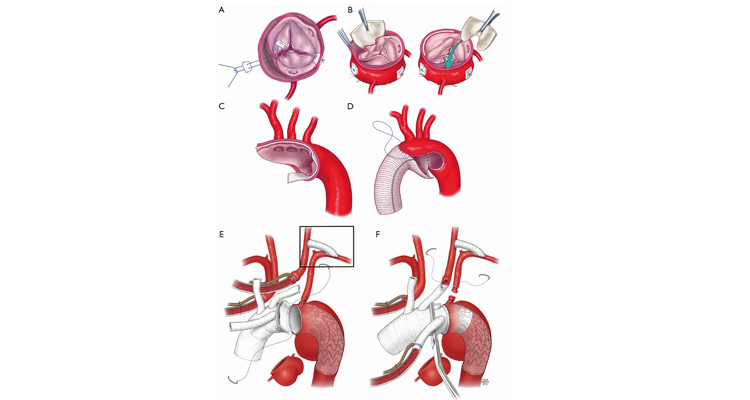
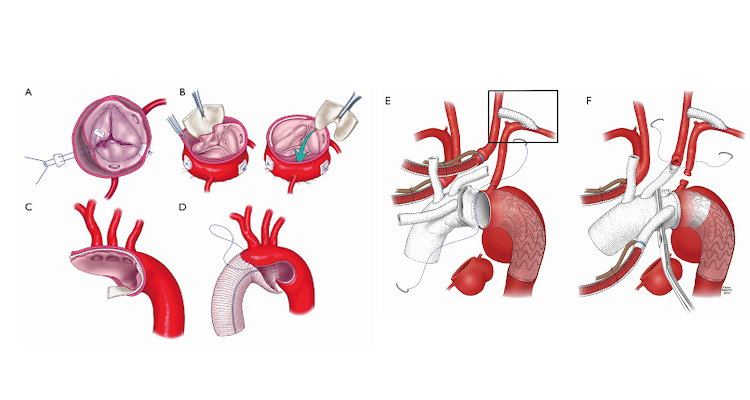
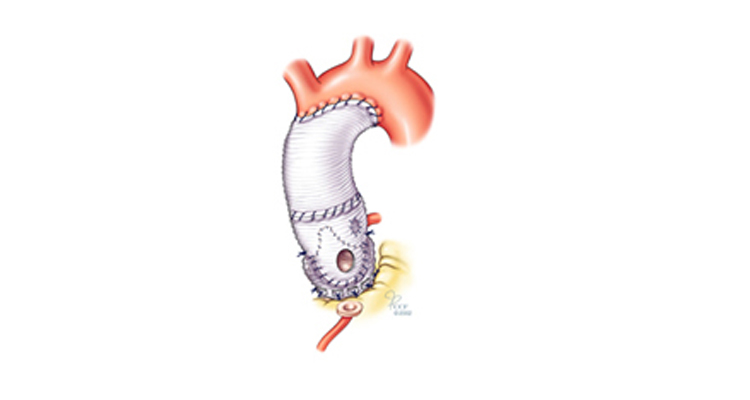
Modified David procedure where the graft is fixed to the level just proximal to the aortic annulus at the left ventricular outflow tract.[114]
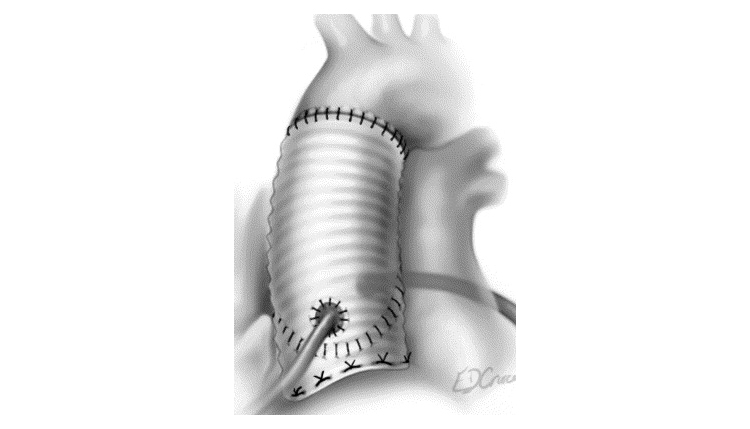
Trimming of the aortic root during modified David Procedure.
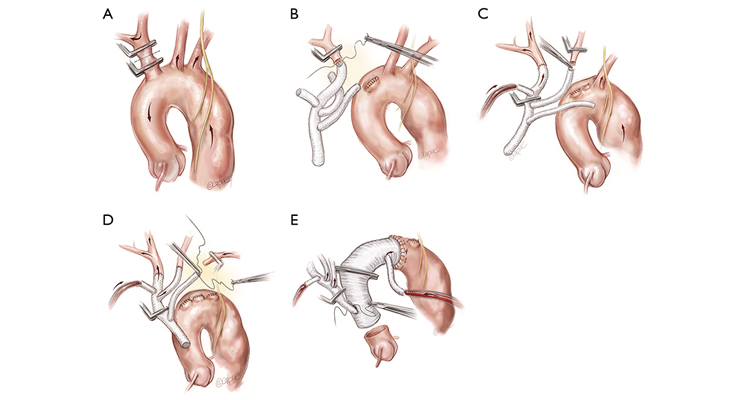
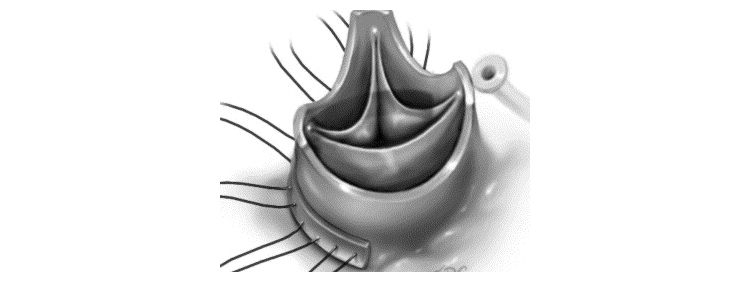
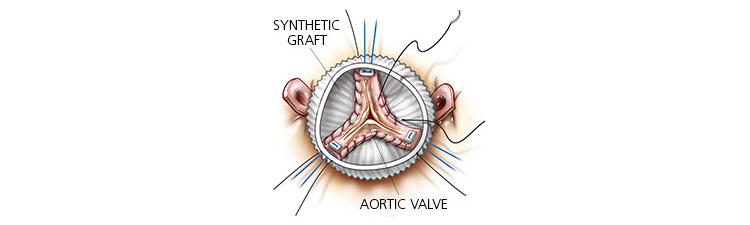
The surgical technique involves resecting all aortic tissue except for a 5mm rim of aorta just above the valve and creating buttons of the coronaries. Dissection is carried proximally below the level of the annulus. Great care must be taken during this portion of the procedure to avoid the RVOT and left atrium. Sutures are then placed from inside the LVOT to outside through the graft for the proximal suture line. The graft is seated and the leaflets are inside the graft. After securing the proximal suture line, the valve leaflets are carefully positioned inside the graft to allow coaptation in the same plane for all three leaflets. The leaflets are then sutured inside the graft by running a suture along the small piece of aortic wall and attaching it to the graft. The coronaries are reimplanted and the distal suture line is performed where appropriate. Echocardiography is used to confirm good operation of the leaflets and no aortic insufficiency.
Indications for a valve-sparing procedure are ascending and root aneurysms (>5cm or 4.5cm for patients with Marfan’s) with normal aortic leaflets. Typically from sinotubular dilatation there is central aortic insufficiency which is easily corrected by this procedure. Asymmetric regurgitation may require leaflet repair. This is an excellent operation for patients with Marfan’s, as it obviates the need for long-term anticoagulation. Recently it has been used in patients with acute Type A aortic dissection who require a root replacement.
Long-term results of this are been excellent. Ten-year survival for patients undergoing valve-sparing techniques ranges from 82-97%..
Subpopulations that have undergone valve-sparing technique include the elderly and those patients with Marfan’s. One study in older patients (>60 years old) demonstrated good results. The peri-operative mortality of 63 patients undergoing valve-sparing replacement was 1.4% with an overall 51 month survival of 84%.
Immediate post-operative and long-term results for Marfan’s patients are also excellent. Volguina et al analyzed the short-term results of 105 patients with Marfan’s who underwent valve-sparing technique.
David et al analyzed the long-term results of their 103 person cohort. Fifteen year survival was 87% and 89% of those alive at fifteen years and patients were free of clinically significant aortic regurgitation.